


Sexually transmitted infections
New sexual partnerships and unprotected intercourse is relatively common amongst travellers. Read about some of the risks to consider

Key messages
-
Sexually transmitted infections (STIs) are a group of viral, bacterial and parasitic infections; while many are treatable, some can lead to complications or serious illness.
-
It has been estimated that 10-20 percent of individuals will have a sexual encounter with a new partner whilst abroad. Increased sexual risk taking abroad is often linked to alcohol use.
-
The incidence rates for some STIs (including the blood-borne viruses hepatitis B and HIV which may be transmitted sexually) are significantly higher in many low-income countries compared to the UK.
-
Those travelling without a steady partner should be aware of the risks, casual sex abroad often happens, even when it is not planned. Reliable condoms should be carried and used to reduce the risks.
-
Those who are concerned that they may have been exposed to an STI are advised to undergo screening tests with their GP centre or a genito-urinary medicine (GUM) clinic. Some STIs can be present without symptoms occurring.
Overview
Sexually transmitted infections (STIs) are a group of viral, bacterial and parasitic infections that are predominantly transferred during sexual intercourse or intimate contact. The World Health Organization (WHO) estimates that more than one million people develop a STI every day and approximately 374 million people acquire one of four STIs: chlamydia, gonorrhoea, syphilis and trichomoniasis each year [1]. The burden of STIs is greatest in low-income countries [2]. Although many STIs are treatable, they may lead to chronic diseases, AIDS, pregnancy complications, infertility, cervical cancer and death [3].
New sexual partnerships and unprotected intercourse is relatively common amongst travellers [4-6] and they contract a wide range of STIs [7, 8]. The risk of developing an STI is thought to be increased in people who have casual sex abroad [4]. Increased sexual risk taking abroad is often linked to alcohol use [9, 10]. There is, however, limited information about effective strategies to prevent the risk of STI acquisition during foreign travel [4, 11].
Disease information
STIs are caused by more than 30 different bacteria, viruses and parasites [1].
Some of the infections that may be transmitted sexually include:
- Chancroid (Haemophilus ducreyi)
- Chlamydia (Chlamydia trachomatis)
- Donovanosis (granuloma inguinale) (Klebsiella)
- Genital herpes (herpes simplex 1 and 2)
- Genital warts (human papillomavirus)
- Gonorrhoea (Neisseria gonorrhoeae)
- Hepatitis A (hepatitis A virus) (usually transmitted by contaminated food and water)
- Hepatitis B (hepatitis B virus, HBV)
- Hepatitis C (hepatitis C virus)
- Human Immunodeficiency Virus (HIV)
- Lymphogranuloma venerum (Chlamydia trachomatis L1, L2, L3)
- Scabies (Sarcoptes scabiei)
- Syphilis (Treponema pallidum)
- Trichomoniasis (Trichomonas vaginalis)
Viral infections
Genital herpes (Herpes simplex 1 and 2)
Genital herpes is common and is found worldwide. It is caused by either Herpes simplex virus 1 or 2 (HSV-1, HSV-2). The virus can infect the mucous membranes and surrounding skin of the genital tract, rectum, mouth, and the throat.
Transmission occurs during close physical contact with a person who has active infection and symptoms occur about 14 days after exposure. The initial infection may present as a 'flu-like' illness, with multiple painful genital ulcers and regional lymphadenopathy (swollen lymph glands). Genital and skin lesions usually begin with a painful papule that progresses to a blister and then ulcerates. On mucous membranes ulceration may appear first. In females the cervix may be involved, and with receptive anal intercourse there may be rectal infection with proctitis (inflammation of the lining of the rectum). Serious complications include meningitis (infection of the membranes that surround the brain and spinal cord) and urinary retention (inability to empty the bladder).
After the initial infection, there can be clinical resolution or occasional recurrence of lesions and symptoms. Recurrent infection may be without symptoms, particularly in women.
Ulcers from active herpes virus infection can increase the risk of HIV transmission [12].
Infants born to mothers who have active genital HSV infection can be infected during delivery. Infected newborns may develop skin lesions, pneumonia, and/or have neurological complications. Women with active genital herpetic lesions, therefore, usually have their babies delivered by caesarean section.
Primary and recurrent genital HSV infection can be treated with anti-viral drugs. These drugs do not eradicate the virus, which remains dormant and may become active at a later date.
Genital warts (human papillomavirus)
There are approximately 100 types of human papillomavirus (HPV), of which about 40 infect the genital tract [13]. Although most infections are without symptoms and self-limiting, genital infection with HPV is associated with genital warts and anogenital cancers in both men and women. Certain HPV types are classified as 'high- risk' depending on their association with the development of cancer. HPV-16 and 18 in particular have been associated with the development of cervical intra-epithelial neoplasia (changes in the cells on the surface of the cervix) which can progress to cervical cancer. HPV infection with 'high-risk' types is also associated with other less common cancers such as cancer of the vulva, vagina, penis, anus and some cancers of the head and neck [14].
Most people who have HPV infection do not develop symptoms (i.e. a visible wart). If genital warts do appear, it can be from two weeks to eight months after sexual contact with an infected partner. In females, warts can occur around the vulva, the tissue around or inside the anus, inside the vagina and on the cervix. In males, the penile shaft and the tissue around the anus are the mostly commonly affected sites, however warts may occur inside the urethral opening and in the rectum.
Infants born to mothers who have genital HPV infection affecting the cervix or vagina, can be infected during delivery and develop anogenital warts or laryngeal papillomas (where growths form in the airway and voice box).
Genital warts are treated with topical preparations (either cytotoxic or immunomodulating agents). Cryotherapy, electrocautery or laser ablation is indicated where there are extensive lesions.
Vaccinations against certain strains of HPV are included in child and adolescent immunisation programmes in a number of high-income countries, including the UK plus some low- and middle-income countries [2, 14, 15]. The vaccine is available on the NHS for young people aged under 25 years. The vaccine is also available for gay, bisexual and other men who have sex with men (GBMSM) up to 45 years of age through sexual health clinics. From 1 September 2023, the vaccination programme will change from a 2-dose to a one-dose schedule for those under 25 years of age. For GBMSM aged 25 or over, 2 doses of vaccine will continue to be offered. For those living with HIV, 3 doses will be offered, irrespective of their age.
The HPV vaccination has been offered to girls in the UK since Sept 2008. From September 2019, boys were included in the routine adolescent vaccination programme. Young heterosexual men who have not been vaccinated through the national programme benefit from herd immunity in the UK as many young women are vaccinated. However those with new sexual partners overseas, from countries where there is no vaccination programme, will not benefit from this protection.
Condom use is recommended as it reduces (but does not eliminate) the risk of transmission [14]. HPV vaccine is also available privately.
Human Immunodeficiency virus (HIV) & Acquired Immune Deficiency Syndrome (AIDS)
HIV infection occurs worldwide; in 2012 there were approximately 35.3 (range 32.2–38.8) million people living with HIV [12]. The prevalence is highest in Sub-Saharan Africa, with nearly one in every 20 adults infected with the virus. Sixty nine percent of all people living with HIV are living in this region [12].
HIV is a lentivirus within the retrovirus family, and there are at least two variants of HIV (HIV-1 and HIV-2). Both types are genetically different and are divided into subsets or clades, with certain subsets endemic to particular geographical areas. HIV-2 is largely confined to West Africa and the Indian sub-continent.
HIV infects lymphocytes and macrophages (white blood cells) that are crucial to effective immunity against a wide variety of infections. Without effective antiretroviral therapy (ART), progressive damage to the immune system over months to years results in an immune system that is unable to fight certain infections and cancers leading to a diagnosis of AIDS.
HIV is transmitted during unprotected sexual contact, through exchange of body fluids, during injecting drug use, and from receipt of unscreened blood products. The presence of co-existing STIs, especially those that result in genital ulceration, is an enhancing factor in HIV sexual transmission. HIV is not transmitted through casual person-to-person contact; air, food, or water; contact with inanimate objects; or by mosquitoes or other insects. The use of any public conveyance (such as airplanes, automobiles, boats, buses, or trains) by people with HIV infection does not pose a risk of HIV infection for other travellers.
About six to eight weeks after exposure to the virus, some persons will develop a self-limited acute retroviral syndrome with fever, muscle pain, lymphadenopathy (swollen lymph glands), mouth ulcers, sore throat, and rash. The infection can then remain latent (dormant) for months or years and not diagnosed until presentation with symptoms associated with immune dysfunction (symptomatic HIV infection or AIDS). Symptomatic HIV infection presents with a wide range of symptoms and signs and any system in the body can be affected. Typical manifestations of AIDS include gastrointestinal problems (weight loss, wasting, diarrhoea), respiratory disease (Pneumocystis pneumonia), skin complaints (such as itching, rash or, mouth ulcers) and central nervous system infection (cryptococcal meningitis and toxoplasmosis). In advanced disease there may be blood disorders (anaemia, neutropenia, and thrombocytopenia) and central nervous system involvement (dementia, neuropathy).
HIV infection can be transmitted from mother to child either in the womb or perinatally (just before, during or soon after birth). Breast-feeding increases the risk of infection. HIV can also be transmitted via contaminated blood or blood products, contaminated syringes and during procedures in which contaminated medical instruments are used (e.g. tattooing, body piercing).
People living with HIV can expect a nearly normal life span if they are diagnosed early, treated promptly and receive regular check-ups. HIV infection is progressive unless treated with effective antiretroviral therapy (ART). Effective ART can suppress viral replication and consequently reduce morbidity from the disease and increase life expectancy [16, 17]. There is increasing access to ART in low-income countries of the world [12].
In the UK, the number of heterosexuals diagnosed with HIV who acquired their infection abroad has more than halved, with 1,430 (48 percent) in 2011 compared to 2,990 (73 percent) in 2002 [18].
Bacterial infections
Chancroid
Chancroid is a common cause of genital ulceration in tropical countries, particularly Africa, Southeast Asia, and Papua New Guinea. It is caused by the bacillus Haemophilus ducreyi and is transmitted through unprotected sex. Men are most commonly affected. For more information about chancroid see the British Association for Sexual Health and HIV (BASHH) patient information leaflet here.
Chlamydia (Chlamydia trachomatis)
See also: Lymphogranuloma venereum (LGV)
Chlamydia is a very common bacterial STI which occurs worldwide and is caused by the bacteria Chlamydia trachomatis (CT). It is transmitted by unprotected vaginal, oral or anal sex or genital contact with an infected partner. In a UK survey in 2010-2, the estimated prevalence in women aged 16-44 years was 1.1 percent for those reporting one partner in the last year and 3.7 percent in those reporting three or more partners in the last year [19].
Infection with CT often causes no symptoms particularly in women. Symptoms may occur 6-19 days after infection and include urethritis (inflammation of the tube that carries urine from the bladder out of the body) which is the usual presenting symptom in males. CT pharyngitis (inflammation of the back of the throat) and proctitis (inflammation of the rectum) are not uncommon in men who have sex with men. In females, the only symptom may be increased vaginal discharge. CT can cause pelvic inflammatory disease and irreversible damage to the fallopian tubes. This may result in an increased risk of ectopic pregnancy or infertility.
Infants born to mothers who have active chlamydial infection can be infected during delivery. Perinatal infection may result in a mild self-limiting conjunctivitis (ophthalmia neonatorum). Chlamydial pneumonitis (inflammation of the lung) is a more serious complication, occurring between the ages of six weeks and three months. Chlamydial infections are treated with antibiotics [20].
Donovanosis (granuloma inguinale)
Donovanosis is a tropical disease found in diverse areas of the world, most of which have limited medical research capabilities. It is caused by the bacillus Klebsiella granulomatis. Recent accurate data for endemic areas are limited [21]. The condition also occurs in commercial sex workers in poor socio-economic conditions. Donovanosis is rare in high-income countries.
More information about Donovanosis here.
Gonorrhoea (Neisseria gonorrhoeae)
Gonorrhoea is one of the most prevalent STIs in the tropics [22] but is also common worldwide. Antimicrobial resistance has become a worldwide problem, and the WHO have developed a global action plan to help curb the spread of antimicrobial resistant Neisseria gonorrhoeae and to prolong the useful life of current treatments [23].
In England and Wales, between July and September 2012 data from 25 collaborating genitourinary medicine (GUM) clinics showed that of 1,518 people diagnosed with gonorrhoea, 12.4 percent reported having a sexual contact outside of the UK. Of those reporting having a sexual contact abroad, 33.6 percent had a sexual contact in Western Europe and 12.1 percent in Eastern Europe [23]. Those who reported sexual contact outside the UK were twice as likely to acquire strains that were resistant to antibiotics [23].
Gonorrhoea is caused by Neisseria gonorrhoeae and can cause infection of the male and female urogenital tract, the rectum, the throat and the eyes. Infection of the throat and rectum is common in men who have sex with men (MSM), these infections often cause no symptoms. Up to 50 percent of women and 10 percent of men with genital infection have no symptoms.
Symptomatic gonorrhoea presents after a two-to-seven-day incubation period. Men develop a purulent penile discharge. Untreated gonococcal infection in men may lead to epididymitis (inflammation of the coiled tube at the back of the testicle) and urethral stricture (narrowing of the urethra). In women symptoms may include vaginal discharge, pain or discomfort while passing urine and post-coital bleeding (bleeding that occurs immediately after sexual intercourse). Untreated infection in women may result in infection and subsequent fallopian tube damage, ectopic pregnancy or infertility. Disseminated gonococcal infection manifesting as gonococcal arthritis, meningitis or endocarditis, occurs in a small number of cases.
Infants may be infected during delivery. Perinatal infection may result in an acute conjunctivitis occurring in the first month of life (ophthalmia neonatorum).
Treatment is with antibiotics but will depend on gonococcal resistance; due to widespread resistance to ciprofloxacin, tetracyclines and penicillins, these agents are no longer reliable. UK treatment guidelines are available on the British Association for Sexual Health and HIV website [24].
Lymphogranuloma venereum (LGV) (Durand-Nicholas-Favre disease, Tropical bubo)
LGV is highly prevalent in parts of Africa, Asia and South America [25]; and is rare in western Europe but outbreaks have occurred amongst men who have sex with men since 2003. In the Health Protection Agency data shows a decrease in cases from 2011 with 395 cases reported in 2012 [26].
LGV is caused by the invasive L1, L2 and L3 serovars of Chlamydia trachomatis. It is transmitted during sexual contact.
More information about LGV here.
Shigellosis
Shigellosis is a gastrointestinal infection (diarrhoeal illness) caused by Shigella bacteria. It is caught by bacteria in faeces being ingested (swallowed) which can occur during sexual contact by direct oral contact or via contaminated objects. The symptoms include diarrhoea, often with blood in it, stomach cramps and fever. Symptoms usually resolve within five to seven days. Treatment decreases the duration of symptoms and may reduce the risk of the infection spreading to others. The European Centre for Disease Control and Prevention have reported on the spread of multi-drug resistant Shigella in the EU/EEA among gay, bisexual and other men who have sex with men (GBMSM). Advice on Shigella for GBMSM is available in a leaflet.
Syphilis
Syphilis occurs worldwide and is caused by the spirochete bacterium Treponema pallidum. Untreated, syphilis has primary, secondary and tertiary phases. It is transmitted both sexually and from mother to child in the womb. The primary lesion, a painless, highly infectious ulcer (chancre), occurs at the site of infection 10-70 days after exposure. The lesion occurs on the external genitalia or may be hidden internally in the vagina, rectum or mouth. Primary lesions gradually heal without treatment. Three to six weeks after the primary infection a secondary phase begins. Symptoms include a classic maculo-papular rash involving the palms of the hands and soles of the feet, generalised lympahadenopathy and meningitis. Untreated, the illness may become dormant, recurring weeks, months or even years after the primary infection (tertiary syphilis).
Congenitally infected infants may be stillborn or develop manifestations of congenital syphilis during the neonatal period or during the first three months of life. Early syphilis in infancy may manifest as a failure to thrive, snuffles, rash, bone abnormalities, hepatosplenomegaly (enlarged liver and spleen) and anaemia. Pre-natal screening and treatment of sero-positive mothers is effective in preventing congenital syphilis [22, 27].
Syphilis is treated with antibiotics.
Parasitic infections
Trichomoniasis (Trichomonas vaginalis)
Trichomoniasis is prevalent worldwide and is caused by the flagellated protozoan parasite Trichomonas vaginalis (TV). It is transmitted during sexual contact. The infection is more common in females and may cause no symptoms. Those with symptoms may experience vaginal itch with a frothy vaginal discharge. Infected men are usually asymptomatic (without symptoms), although they may complain of urethral discharge and urinary discomfort.
Infants born to mothers who have active TV infection may be infected during delivery.
TV is treated with antibiotics.
Scabies (Sarcoptes scabiei)
Scabies occurs worldwide,and is common in poor socio-economic conditions. It is caused by a parasitic mite (Sarcoptes scabiei) that thrives in conditions where people live in close proximity. It can also be transmitted from person to person during sexual contact. Mite infestation manifests as intensely itchy, nodular lesions, commonly between the fingers and toes, abdomen, armpit and groin. Secondary infection is common.
Hyperkeratotic (Norwegian) scabies, is a particularly contagious and severe form of the disease, characterised by thick plaques or crusts and found on the face, scalp, back, buttocks, nails and feet.
Scabies is treated either with topical anti-parasitics or orally with an antiparasitic drug such as ivermectin. Hyperkeratotic scabies usually requires a combination of topical preparations and oral medication. For up to date information see link in the treatment section below.
Risk areas
STIs occur throughout the world, but the incidence rates for some STIs including the blood-borne viruses hepatitis B and HIV are significantly higher in many low-income countries. According to the WHO, low- and middle-income countries lag far behind in providing services for diagnosis and treatment of STIs [2]. See Figure 1 below for estimated numbers of new cases of some of the curable STIs worldwide and Figure 2 for the estimated prevalence of HIV infection in adults.
Figure 1: Estimated new cases of curable sexually transmitted infections (gonorrhoea, chlamydia, syphilis and trichomoniasis) by WHO region, 2008

Source: World Health Organization, Sexually transmitted infections fact sheet [1]
Figure 2: Estimated prevalence rate of HIV infection in adults, 2014
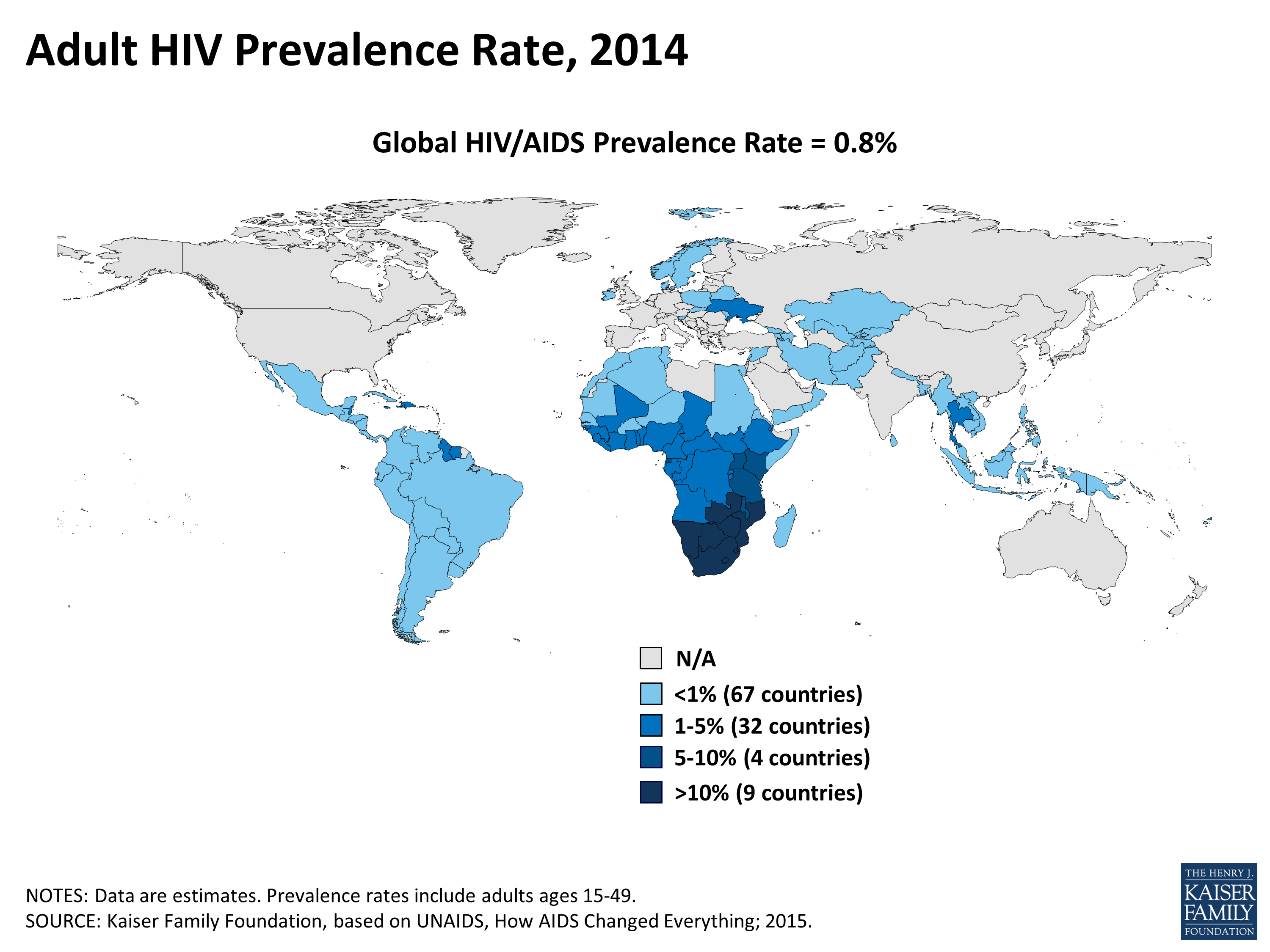
Source: Kaiser Family Foundation [27]
Risk for travellers
STI risk in travellers is dependent on their behaviour (e.g. unprotected sexual intercourse or other intimate contact) and the prevalence of STIs in the contact population. Sexual risk-taking may be influenced by many factors, including change in social environment and substance or alcohol use [9, 29].
It has been estimated that 10-20 percent of individuals will have a sexual encounter with a new partner whilst abroad [4, 5, 9]. Up to 50 percent of people engaging in new sexual relationships abroad do not consistently use condoms [4]. Younger travellers are more likely to have a sexual encounter with a new partner abroad [4, 9]. In a 2010 review article the predominant characteristics of people who had new sexual partners abroad were found to be: young age, male gender, single status, and travelling alone or with friends, with a previous history of multiple sexual partners or an STI [4]. Those who travel or stay abroad for longer periods and men who have sex with men are at higher risk of developing new sexual partnerships and having unprotected intercourse [4].
Other groups of travellers known to be at increased risk of STIs include seafarers, military personnel, long distance lorry drivers, business travellers, migrant workers, expatriates and those visiting friends and family [4, 8, 30-33]. Some people, both men and women, travel specifically for the purpose of engaging in sexual activity [34]. The prevalence of STIs, such as HIV-infection and gonorrhoea, is high in sex workers (SWs) and local populations who frequently have sex with tourists. Travellers who seek SWs, including those who travel as 'sex tourists', are at high risk of exposure to STIs [30, 33, 35, 36].
Transmission
Transmission of STIs occurs during unprotected sexual intercourse (oral, vaginal or anal) or intimate skin-to-skin contact.
Some organisms (HIV, hepatitis B and C viruses and syphilis) can also be transmitted via contaminated blood or blood products, contaminated syringes and during procedures in which contaminated medical instruments are used (e.g. dental procedures, tattooing, body piercing).
Although rare hepatitis A can also be transmitted sexually or by blood transfusion and by transfusion of blood products.
Shigella dysentery (an infection causing diarrhoea, stomach cramps and flu like symptoms) can also be transmitted sexually, cases have been reported in men who have sex with men (MSM) [37].
Organisms can also be transmitted from mother to child during pregnancy (HIV, syphilis, and HBV), during childbirth (HIV, gonorrhoea, syphilis, herpes, chlamydia, HBV) or during breast-feeding (HIV).
Signs and symptoms
The symptoms of the different STIs vary with each infection (see details in the overview section). Some STIs may not lead to symptoms.
Diagnosis and treatment
Testing for STIs is confidential and available at GP surgeries or local genito-urinary medicine (GUM) clinics. Many of the STIs are treatable and early diagnosis and treatment can prevent complications developing.
Individuals who have been at high risk of exposure to an STI during travel should seek medical advice and post exposure screening at the earliest opportunity. Further sexual contact should be avoided until screening tests for STIs have been performed and are negative.
UK treatment and management guidelines for STIs are available from British Association for Sexual Health and HIV.
In certain circumstances, post-exposure prophylaxis following potential sexual exposure to hepatitis B and HIV may be appropriate [38].
Preventing STIs
Travellers should be counselled about the risk of acquiring STIs during international travel.
Studies have highlighted that although travellers usually have adequate knowledge of STIs and HIV, they often do not perceive any personal risk of STI acquisition. A few studies have shown that STI prevention advice did not motivate behaviour change and reduce sexual risk-taking activity in travellers [4, 11]. However, in another study the recall of reading STI information appeared to be related to more consistent condom use [39].
The authors of a 2014 review article [11] suggest including some information on STIs in the pre-travel consultation for travellers at risk (those travelling without a steady partner) including:
- The fact that casual sex abroad often happens, even when this is not planned.
- The recommendation that condoms are taken abroad (this was found to be an independent predictor of protected casual sex).
- Written information focusing on both prevention and post-exposure management.
Abstinence from sexual intercourse with a new or known to be infected partner is the most effective strategy for preventing HIV infection and other STIs, but this could be a challenge for some travellers.
Condoms
Studies have demonstrated that male and female condoms offer effective protection against STIs, including HIV, but only when used consistently and correctly [40-42].
In the UK, condoms should carry the BSI or CE kite-mark. Travellers from the UK should carry an adequate supply of condoms of this standard. For travellers buying condoms overseas, the following should be considered:
- Check that condoms carry a recognised mark of quality e.g. European kite-mark BSEN 600, International Standards Organisation (ISO) mark or approval by the Food and Drug Administration (FDA).
- Male condoms are available worldwide and female condoms are available in many countries.
- Counterfeit condoms may be available in some locations, and these may also carry the quality marks. Counterfeit condoms may fail to protect against STIs or unwanted pregnancy. Male condoms manufactured in South and Southeast Asia are made slightly narrower than those available in the UK.
- Condoms should not be used beyond the marked expiry date.
- Contraception may be difficult to obtain in some countries due to cultural or religious opposition, poor quality of available services, users and providers bias and gender-based barriers [43].
Emergency contraception overseas
Emergency contraception may sometimes be required. Emergency contraception using hormones is usually effective if given within 72 hours of unprotected intercourse. This method may be available in many countries. Insertion of an intrauterine contraceptive device (IUCD) within five days of unprotected intercourse may prevent a pregnancy. This method is inadvisable in some countries because of the risks associated with invasive procedures.
Vaccine information
Hepatitis B vaccination can be offered to provide protection against the transmission of this virus. A course of three injections can be provided. For more information see hepatitis B in brief.
The human papilloma virus (HPV) vaccine is currently offered to young people aged 12-13 in the UK. Young people are eligible until their 25th birthday. In addition to the routine adolescent programme, there is also a separate HPV vaccination programme for GBMSM aged up to 45 years, which is delivered through sexual health clinics [43].
From 1 September 2023, the vaccination programme will change from a 2-dose to a one-dose HPV schedule for those aged under 25 years. GBMSM aged 25 or over will continue to be offered 2 doses. Individuals living with HIV will be offered 3 doses, irrespective of their age. [14, 43].
Resources
- Rape and sexual assault abroad. The Foreign, Commonwealth & Development Office
- British Association for Sexual Health and HIV
- Marie Stopes International
- HIV and AIDS
- British HIV Association
- The Terence Higgins Trust
References
-
World Health Organization, Sexually transmitted infections, fact sheet 110, updated 10 July 2023. [Accessed 27 July 2023]
-
World Health Organization, Sexually transmitted infections (STIs): The importance of a renewed commitment to STI prevention and control in achieving global sexual and reproductive health. [Accessed 27 July 2023]
-
World Health Organization, 10 facts on sexually transmitted infections. October 2008. [Accessed 21 August 2015]
-
Vivancos, R. Abubakar, I., Hunter, P.R. Foreign travel, casual sex, and sexually transmitted infections: systematic review and meta-analysis. International Journal of Infectious Diseases 14, 2010: e842-e851.
-
Bhatta, P., Simkhada P., Teijlingen E.V. Maybin S. A Questionnaire Study of Voluntary Service Overseas (VSO) Volunteers: Health Risk and Problems Encountered. Journal of Travel Medicine 2009; Volume 16 (Issue 5): 332-337
-
Richens, J. Sexually transmitted infections and HIV among travellers: A review. Travel Medicine and Infectious Disease (2006) 4, 184-195
-
Ansart S. Hochedez, P., Perez, L. et al. Sexually Transmitted Diseases Diagnosed Among Travelers Returning from the Tropics. Journal of Travel Medicine 2009; Volume 16 (Issue 2): 79-83
-
Matteelli, A., Schlagenhauf, P., Carvalho A.C.C. et al Travel-associated sexually transmitted infections: an observational cross-sectional study of the GeoSentinel surveillance database. Lancet Infectious Diseases, Volume 13, Issue 3, Pages 205-213, March 2013
-
Vivancos, R., Abubakar, I., Hunter P.R. Foreign travel associated with increased sexual risk-taking, alcohol and drug use among UK university students: a cohort study. Int J STD AIDS 2010, 21: 46 Accessed 17 April 2014]
-
Cabada, M.,M., Mozo, K. Pantenburg, B, Gotuzzo, E. Excessive alcohol consumption increases risk taking behaviour in travellers to Cusco, Peru. Travel Medicine and Infectious Disease (2011) 9, 75e81
-
Croughs, M. Remmen R., Van den Ende, J. The Effect of Pre-Travel Advice on Sexual Risk Behavior Abroad: A Systematic Review. Journal of Travel Medicine 2014; Volume 21 (Issue 1): 45-51
-
World Health Organization, HIV/AIDS fact sheet, July 2015, [Accessed 21 August 2015]
-
McCance DJ (2004) Papillomaviruses. In: Zuckerman AJ, Banatvala JE, Pattison JR, Griffiths P and Schoub B (eds) Principles and practice of clinical virology. 5th edition. Wiley & Sons Ltd.
-
UK Health Security Agency, Human Papillomavirus Chapter 18a in Immunisation against infectious disease. 20 June 2023 [Accessed 27 July 2023]
-
World Health Organization, Scaling up HPV vaccine introduction, December 2016 [Accessed 13 August 2019]
-
Nakagawa F, Lodwick RK, Smith CJ et al. Projected life expectancy of people with HIV according to timing of diagnosis. AIDS 2012; 26: 335-343.
-
May M, Gompels M, Delpech V et al. Impact on life expectancy of HIV-1 positive individuals of CD4+ cell count and viral load response to antiretroviral therapy: UK cohort study. AIDS 28(8): 1193-1202. 15 May 2014 [Accessed 21 August 2015]
-
Public Health England, HIV in the United Kingdom 2013 report, [Accessed 17 April 2014]
-
Sonnenberg, P. Clifton S., Beddows,S et al Prevalence, risk factors, and uptake of interventions for sexually transmitted infections in Britain: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal), Lancet Vol 382, No 9907, p1795-1806, 30 November 2013 [Accessed 21 August 2015]
-
Public Health England, Genital Chlamydia Trachomatis, general information. [Accessed 21 August 2015]
-
O'Farrell, N. Donovanosis. Sex Transm Infect. 2002;78:452-457. [Accessed 21 August 2015]
-
Mabey, D., Richens, J. Sexually transmitted infections (Excluding HIV). In: Cook GC, Zumla A. Eds. Manson's Tropical Diseases.21st Edition. 2003 Saunders.427-456
-
Public Health England, GRASP 2012 report, The Gonococcal Resistance to Antimicrobials Surveillance Programme, October 2013. [Accessed 21 August 2015]
-
British Association for Sexual Health and HIV, Guidelines. [Accessed 21 August 2015]
-
Public Health England, LGV (Lymphogranuloma venereum) [Accessed 21 August 2015]
-
Health Protection Agency, Health Protection Report. Vol 5, No 24, 17 June 2011. [Accessed 21 August 2015]
-
Chakraborty, R., Luck, S. Syphilis is on the increase: the implications for child health. Arch Dis Child. 2008; 93:105-9.
-
Kaiser Family Foundation, The global HIV/AIDS epidemic, 31 July 2015. [Accessed 21 August 2015]
-
Tveit, KS, Nilsen A, Nyfors A. Casual sexual experience abroad in patients attending an STD clinic and at high risk for HIV infection. Genitour Med. 1994; 70:12-14.
-
Ward, B.J., Plourde, P. Travel and Sexually transmitted infections. Journal of Travel Medicine, Volume 13, Issue 5, 2006, 300-317.
-
Mulhall, B.P. Sex and travel: studies of sexual behaviours, disease and health promotion in international travellers- a global review. International Journal of STD & AIDS 1996; 7:455-465.
-
Richens, J. Sexually transmitted infections and HIV among travellers: A review. Travel Medicine and Infectious Disease, Volume 4, Issues 3-4, May-July 2006, 184-195
-
Memish ZA, Osoba AO. Sexually transmitted diseases and travel. Int. J. Antimicrob Agents. 2003 Feb;21(2):131-134
-
Bauer, I.L., Romance tourism or female sex tourism? Travel Medicine and Infectious Disease, 2014; 12: 20e28.
-
Cabada, M.M., Echevarria, J.I., Seas, C. Gotuzzo, E., High Prevalence of Sexually transmitted infections Among Young Peruvians Who Have Sexual Intercourse With Foreign Travelers in Cuzco. Journal of Travel Medicine 2009; Volume 16 (Issue 5) 299-303.
-
Wong, W.C.W. Yim, Y.L., Lynn H. Sexually transmitted infections Among Female Sex Workers in Hong Kong: The Role of Migration Status. Journal of Travel Medicine 2011; Volume 18 (Issue 1): 1-7.
-
Public Health England, Shigella dysentery on the rise among gay and bisexual men. 30 January 2014. [Accessed 21 August 2015]
-
Benn, P. Fisher M. Kulasegaram R. on behalf of BASHH. UK guideline for the use of post-exposure prophylaxis for HIV following sexual exposure (2011) International Journal of STD & AIDS 2011; 22: 695-708 [Accessed 21 August 2015]
-
Croughs, M., Van Gompel A, de Boer E, van den Ende. J. Sexual risk behavior of travelers who consulted a pretravel clinic. J. Travel Med. 2008; 15:6-12.
-
Pinkerton SD, Abramson PR, Turk ME. Updated estimates of condom effectiveness. J Assoc Nurses AIDS Care. 1998 Nov-Dec;9(6):88-9
-
Fontanet, A., Saba,J., Chandelying, V. et al. Protection against sexually transmitted diseases by granting sex workers in Thailand the choice of using the male or female condom: results from a randomized controlled trial. AIDS 1998;12 (14):1851-1859
-
French, P., Latka M., Gollub, E. et al. Use/effectiveness of the female versus male condom in preventing sexually transmitted diseases in women. Sex Transm Dis 2003; 30:433-9.
-
UK Health Security Agency, Vaccine update: issue 339, June 2023 - HPV specialist, 28 June 2023. Accessed 27 July 2023]
-
Shigellosis information added to bacterial infections section and edits made to genital warts, vaccine information. WHO statistic and references updated.
Explore more
Chikungunya
This viral infection occurs in some tropical and subtropical regions of the world, predominantly transmitted through the bite of an infected Aedes
Updated: 12 February 2025Malaria
Malaria is a serious and potentially life-threatening disease, transmitted to humans through the bite of infected female Anopheles spp. mosqu
Updated: 07 January 2025Influenza (flu)
Influenza is a highly infectious, viral infection of the lungs and airways
Updated: 18 December 2024Yellow fever
Yellow fever is caused by a virus, which circulates between infected monkeys or humans and mosquitoes
Updated: 17 October 2024Infectious diseases
Chikungunya
This viral infection occurs in some tropical and subtropical regions of the world, predominantly transmitted through the bite of an infected Aedes mosquito
Updated: 02 February 2018Malaria
Malaria is a serious and potentially life-threatening disease, transmitted to humans through the bite of infected female Anopheles spp. mosquitoes
Updated: 13 February 2024Influenza (flu)
Influenza is a highly infectious, viral infection of the lungs and airways
Updated: 18 December 2024Preparing for healthy travel
Insect and tick bite avoidance
Protection from insect and tick bites is essential to help prevent vector-borne diseases such as malaria, yellow fever and Zika
Updated: 21 March 2024Travel Insurance
Travellers must declare medical conditions when taking out travel insurance to ensure they are suitably covered
Updated: 26 September 2019Special risk travel/traveller
Hajj and Umrah
The Ministry of Health of Kingdom of Saudi Arabia issue their requirements and recommendations for Hajj and Umrah annually
Updated: 15 May 2024Travelling with additional needs and/or disability
This factsheet provides an overview and advice on the points to consider when travelling with additional needs and/or disability
Updated: 06 February 2018Sickle cell disease and thalassaemia
Information on pre-travel preparation, tips to stay health abroad and links to useful resources for travellers with sickle cell disease and thalassaemia
Updated: 19 February 2021Clinic resources
Educational events
A list of courses, conferences and study days of relevance to UK health professionals working, or wishing to work, in the field of travel medicine
Updated: 14 March 2017Vaccines and medicines: availability, supply, shortages and use of unlicensed medicines
Information for health professionals on availability of vaccines and use of unlicensed products
Updated: 17 October 2022The green book travel chapters
UK Health Security Agency Immunisation against infectious disease, the 'green book' travel chapter updates
Updated: 06 February 2024

