


Snake bites and avoidance
Advice for travellers on prevention and management of snake bites

Key messages
-
The snake bite risk for most travellers is low and can be minimised by sensible precautions.
-
If a snake is encountered, advice is to remain calm, remain still, do not threaten the snake and if possible, back off slowly.
-
Half of bites do not result in envenomation (i.e. actual injection of venom).
-
If envenomed, death is unlikely with prompt treatment, splint the bitten limb and evacuate to hospital as a chair/stretcher case.
-
Antivenom is an effective treatment if given in time, however, it may produce a significant allergic reaction so must be used only where medical facilities are capable of managing this.
Overview
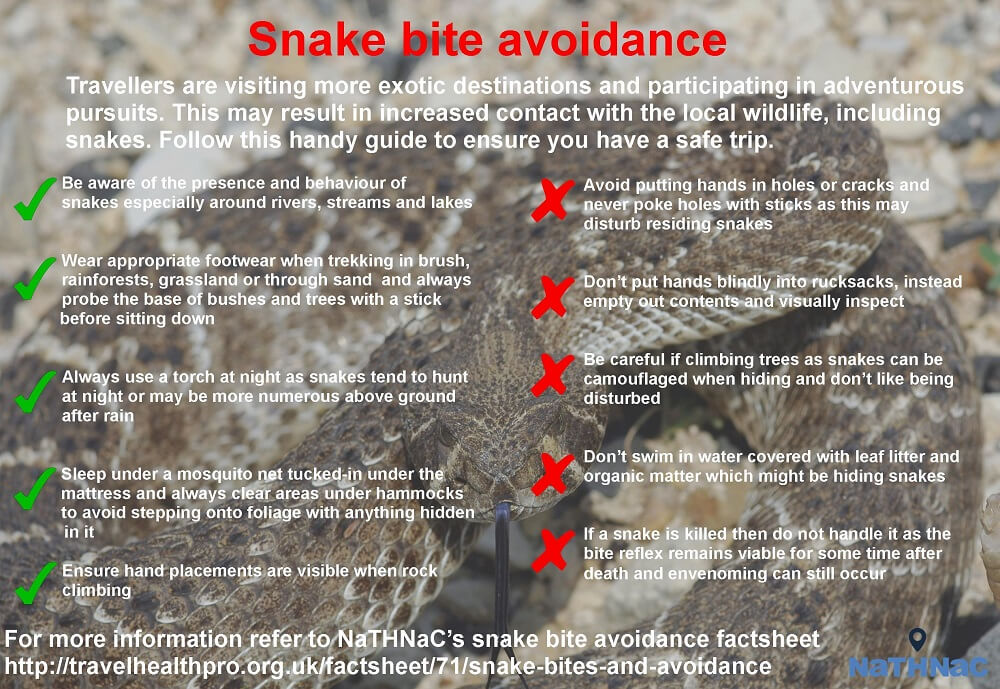
Travellers are visiting more exotic destinations and participating more than ever in adventurous pursuits. This may result in increased inadvertent contact with local wildlife including snakes, scorpions, spiders, jellyfish, and stinging fish. Of these, globally, venomous land snakes are the most important medically [1].
Many animals and flora are poisonous when ingested or inhaled so the term venomous is used when referring to snakes as they actively inject their poison (venom).
Venom
Snake venom is a very complex substance produced by salivary glands and delivered through the bite of a fang. It contains many proteins, enzymes, and toxins which affect different body systems. Each snake species has a specific mix of venom, producing a combination of neurotoxic (affecting the nervous system), haemotoxic (affecting blood or vascular system) or myotoxic (damage to muscles) effects.
Neurotoxic venoms produce muscle weakness often first visible as drooping eyelids but progressing to paralysis including of the breathing muscles.
Haemotoxic venom induces a clotting disorder resulting in bleeding both from the bite wound and more generally in internal organs and tissues.
Some venoms are necrotic, that is, they produce swelling and tissue damage and tissue death. This is often seen first at the site of the bite, but swelling can be significant and affect the whole limb. Some snake bites are very painful, others not.
There are about 3,000 species of snake of which approximately 600 are venomous. The World Health Organization has launched a Snakebite Information and Data platform [2] as part of its global strategy for prevention and control of snake bite envenoming [3]. Snakes are cold blooded and classified into about 20 families of which the most medically important are described below:
Elapids
Elapids have rounded heads which blend into the body with often no distinct neck. Pupils are round and the body is thin with a tapering tail. Fangs are small with a fixed position. All are venomous, with a usually, but not exclusively, neurotoxic venom. Examples include cobras, mambas, kraits, coral and sea snakes.
Vipers
Vipers have diamond shaped heads distinct from the body which is stocky with rapid tapering of the tail. In rattlesnakes the tail forms into a series of scales and the distinctive rattle. Pupils are elliptical. All are venomous with a usually, but not exclusively, haematotoxic venom.
Colubrids
Colubrids are the largest family of snakes with the vast majority being harmless to humans. They include the 'back fanged' snakes where fangs are towards the rear of the mouth. Bites from a few snakes within this group can be fatal such as the South African boomslang, twig snakes and Asian keelback snakes.
Atractaspids
Atractaspids are found in Africa and the Middle East and are commonly known as mole vipers, stiletto snakes and burrowing asps. Most are too small to cause serious envenoming in humans, but their bites can be extremely painful and lead to serious tissue damage. Due to the fang position many can bite sideways and backwards meaning they are difficult to handle.
Boas and Pythons
The boas and pythons, are large non venomous snakes which wrap their muscular coils around prey and kill by constriction preventing breathing and causing crushing.
Snake sensory perception
A snake has poor hearing but is able to track prey by a number of senses including the ability to detect small vibrations in the ground along its underbelly surface. All snakes 'sample' the air by tasting molecules from the environment to detect prey. It is a myth that all snakes have poor vision. Some surface snakes have good eyesight especially for motion sensing and some snakes even have binocular vision. Additionally, the pit vipers, pythons and some boas have infrared receptors in pits either side of the front of the head which allow them to track warm blooded creatures.
Risk to the traveller
Snakes are found in all environments except for a few islands, the Antarctic and permanently frozen areas of the Arctic. They live in desert, rainforest, swamps, grasslands, water, temperate climes and even up to 4,800m in the Asian Himalaya [4]. Snake bite risk is highest where human and snake habitat or activities overlap and predominantly affects the rural working poor such as farmers and hunters and their children. An example would be a barefoot rural farmer tending rice in a paddy field. Risk is particularly high at times of flooding as land snakes share a smaller amount of land with humans [3]. As snakes are cold blooded and thus unable to generate heat internally, they tend to seek out warm environments which may attract them into the human home especially if this is also a source of food such as rodents.
Worldwide, snakes cause considerable death and disability. The World Health Organization have estimated 5.4 million people worldwide are bitten by snakes each year with 1.8 to 2.7 million cases of envenoming, predominantly in Africa, Asia and Latin America. Approximately 81,000 to 138,000 people die each year because of snake bites, and around three times as many amputations and other permanent disabilities are caused by snake bites annually [5].
Travellers are much less likely to come into contact with snakes than local residents, but contact is more likely if staying in basic accommodation where food stuffs are stored attracting rodents, or by undertaking activities in snake areas such as trekking or swimming. Data on snake bite incidence in travellers is not readily available but actual deaths after bites are rare due to the ability of travellers to access prompt modern health care.
Before travel
If undertaking activities which might result in snake encounters, travellers should research the species of snakes in the destination environment and their main characteristics. They should also know where and how long it takes to get to local healthcare facilities likely to have antivenom.
Travel insurance should cover planned activities. Appropriate clothing and footwear such as boots should be packed (see below).
During travel
Snakes are often hidden or camouflaged. Using a local guide may improve detection and avoidance of snakes.
Humans are not prey and snakes tend to detect them by the mechanisms above and will mostly move out of the way if possible. If one is cornered or inadvertently trodden or rolled on it may bite defensively. Some snakes such as mambas (Africa) or fer-de-lance (Central America) have reputations for being more aggressive and prone to attack.
If a snake is encountered, the advice is to remain calm, remain still, do not threaten the snake and if possible, back off slowly. 90 percent of bites are on the limbs particularly the legs down at ankle/lower leg level. The following advice may be helpful for travellers.
Avoiding snake bite
Do:
- Be aware of the presence and behaviour of snakes in the destination area.
- Be cautious especially around rivers, streams and lakes.
- Avoid snake charmers- the snake isn't always under control.
- Wear stout footwear such as walking boots when trekking in brush, rainforests grassland or through sand (some snakes bury themselves with just their heads above sand level and may easily be trodden on).
- Check the base of bushes and trees before sitting down.
- Shake out boots before putting them on.
- Shake out sleeping bags and clothes before using.
- Use a torch at night. Snakes tend to hunt at night or may be more numerous above ground after rain.
- Ensure trails to latrines in forests are well marked and clear underfoot.
- Sleep off the ground in forest areas and huts. Rolling onto a snake whilst sleeping is a common cause of bites. Sleep under a mosquito net tucked-in under the mattress.
- Clear areas under hammocks to bare earth to avoid stepping onto foliage and anything hidden within it.
- Hang rucksacks off the ground and buckle up tightly.
- Wear gardening gloves when collecting wood; wood piles may harbour snakes and scorpions.
- Avoid blindly stepping over logs when walking in snake territory; step up onto logs, look over then step over.
- Ensure hand placements are visible when rock climbing as snakes may be on ledges.
- Store rubbish away from living areas as it will attract rodents and snake predators.
Don't:
- Walk barefoot or in sandals in snake areas including soft sand.
- Put hands in holes or cracks or poke holes with sticks as this may disturb snake residents.
- Put hands blindly down into rucksacks. Instead, empty out contents and visually inspect.
- Climb or shake trees as these may hide snakes especially if camouflaged.
- Swim in water covered with leaf litter and organic matter which might be hiding snakes.
- Disturb or interfere with any snake encountered and definitely do not try to pick it up.
- Do not handle a snake if it is killed as the bite reflex remains for some time after death.
If bitten
Remain Calm! About 50 percent of snake bites overall do not contain any venom and if the wound is envenomed then immediate death is very unlikely usually taking 12- 48 hours. Prompt treatment is very effective. The priority is to get to a hospital facility for professional treatment and administration of antivenom.
Do:
- Move the casualty away from the snake.
- Reassure the casualty of the above.
- Treat any bite as containing venom until proven otherwise.
- Lay the casualty down. They need to remain calm and minimise movement. Movement will encourage the venom to be distributed around the body. Use a stretcher if possible.
- Remove rings and wristbands from the affected limb in case of swelling.
- Pressure bandaging should be avoided. This technique is primarily used in Australia for elapid (neurotoxic) bites [6] but may cause additional harm with other snake species [7, 8]. There are differing opinions of the use of pressure bandaging with some clinicians citing limited benefits with potential for additional harm [9].
- Splint the limb so that it cannot be moved.
Don't:
- Don't try to capture or kill the snake as this may result in further bites. Photograph the snake if it is possible to do so without exposing anyone to further risk.
- Don't interfere with the bite wound in any way.
- Australian snake bite guidelines advise against washing the wound as swabs of the venom are used for identifying the snake and antivenom required [6].
- Do NOT use a tourniquet.
- Don't use suction devices on the wound/electric shocks/wound cutting/snake stones or other 'traditional' remedies [10].
- Don't give aspirin or other anti-inflammatory type painkillers as these can worsen bleeding.
- Don't use antivenom unless there are facilities and expertise to manage any severe allergic reactions.
Spitting cobras
These can project a jet of venom about one metre, usually aimed to the eyes. This can be extremely painful with spasm of the eyelids and intense eye watering. Treatment should initially be washing with plenty of clean water and evacuation to hospital.
Resources
References
-
Junghanss, T. and M. Bodio. Medically important venomous animals: biology, prevention, first aid, and clinical management. Clin Infect Dis, 2006. 43(10): p. 1309-17.
-
World Health Organization. Snakebite Information and Data platform [Accessed 3 December 2024]
-
World Health Organization. Snakebite envenoming - A strategy for prevention and control. 19 May 2019 [Accessed 3 December 2024]
-
Shah, K.B. and S. Tiwari, Herpetofauna of Nepal: A Conservation Companion. Vol. VIII. 2004, Nepal: IUCN - The World Conservation Union.
-
World Health Organization. Snakebite Envenoming Fact sheet 12 September 2023 [Accessed 3 December 2024]
-
The University of Melbourne, Department of Pharmacology and Therapeutics. First aid for snake bites in Australia and New Guinea. (cited 2016 30th December 2016) [Accessed 3 December 2024]
-
Seifert, S., J. White, and B.J. Currie, Pressure bandaging for North American snake bite? No! Clin Toxicol (Phila), 2011. 49(10): p. 883-5 [Accessed 3 December 2024]
-
Maduwage, K, Gamage, S.K, Gutiérrez, J.M. First aid and pre-hospital practices in snakebite victims: The persistent use of harmful interventions. Toxicon Volume 238, 1 February 2024
-
Little, M. Harm due to the use of pressure bandage immobilisation in patients bitten by snakes in Australia. Clinical Toxicology Volume 61, 2023 - Issue 8 [Accessed 3 December 2024]
-
Ralph, R. Managing snakebite. Clinical Update. BMJ 2022; 376 doi: https://doi.org/10.1136/bmj-2020-057926 (Published 07 January 2022) [Accessed 3 December 2024]
Explore more
Diseases spread by insects and ticks in the American continent (the Americas)
Depending on the destination, travellers may be at risk of a number of different diseases
Updated: 15 October 2024Infectious diseases
Chikungunya
This viral infection occurs in some tropical and subtropical regions of the world, predominantly transmitted through the bite of an infected Aedes mosquito
Updated: 02 February 2018Malaria
Malaria is a serious and potentially life-threatening disease, transmitted to humans through the bite of infected female Anopheles spp. mosquitoes
Updated: 13 February 2024Influenza (flu)
Influenza is a highly infectious, viral infection of the lungs and airways
Updated: 18 December 2024Preparing for healthy travel
Insect and tick bite avoidance
Protection from insect and tick bites is essential to help prevent vector-borne diseases such as malaria, yellow fever and Zika
Updated: 21 March 2024Travel Insurance
Travellers must declare medical conditions when taking out travel insurance to ensure they are suitably covered
Updated: 26 September 2019Special risk travel/traveller
Hajj and Umrah
The Ministry of Health of Kingdom of Saudi Arabia issue their requirements and recommendations for Hajj and Umrah annually
Updated: 15 May 2024Travelling with additional needs and/or disability
This factsheet provides an overview and advice on the points to consider when travelling with additional needs and/or disability
Updated: 06 February 2018Sickle cell disease and thalassaemia
Information on pre-travel preparation, tips to stay health abroad and links to useful resources for travellers with sickle cell disease and thalassaemia
Updated: 19 February 2021Clinic resources
Educational events
A list of courses, conferences and study days of relevance to UK health professionals working, or wishing to work, in the field of travel medicine
Updated: 14 March 2017Vaccines and medicines: availability, supply, shortages and use of unlicensed medicines
Information for health professionals on availability of vaccines and use of unlicensed products
Updated: 17 October 2022The green book travel chapters
UK Health Security Agency Immunisation against infectious disease, the 'green book' travel chapter updates
Updated: 06 February 2024


{kind=link}