
General Information
The information on these pages should be used to research health risks and to inform the pre-travel consultation.
Travellers should check the Foreign, Commonwealth & Development Office (FCDO) country-specific travel advice page (where available) which provides information on travel entry requirements in addition to safety and security advice.
Travellers should ideally arrange an appointment with their health professional at least four to six weeks before travel. However, even if time is short, an appointment is still worthwhile. This appointment provides an opportunity to assess health risks taking into account a number of factors including destination, medical history, and planned activities. For those with pre-existing health problems, an earlier appointment is recommended.
All travellers should ensure they have adequate travel health insurance.
A list of useful resources including advice on how to reduce the risk of certain health problems is available below.
Resources
Vaccine Recommendations
Details of vaccination recommendations and requirements are provided below.
All travellers
Travellers should be up to date with routine vaccination courses and boosters as recommended in the UK. These vaccinations include for example measles-mumps-rubella (MMR) vaccine and diphtheria-tetanus-polio vaccine.
Country-specific diphtheria recommendations are not provided here. Diphtheria tetanus and polio are combined in a single vaccine in the UK. Therefore, when a tetanus booster is recommended for travellers, diphtheria vaccine is also given. Should there be an outbreak of diphtheria in a country, diphtheria vaccination guidance will be provided.
Those who may be at increased risk of an infectious disease due to their work, lifestyle choice, or certain underlying health problems should be up to date with additional recommended vaccines. See details on the selective immunisation programmes and additional vaccines for individuals with underlying medical conditions at the bottom of the 'Complete routine immunisation schedule' document and the individual chapters of the 'Green Book' Immunisation against infectious disease for further details.
Certificate requirements
Please read the information below carefully, as certificate requirements may be relevant to certain travellers only. For travellers further details, if required, should be sought from their healthcare professional.
- There is no risk of yellow fever in this country, however, there is a certificate requirement.
- Under International Health Regulations, proof of vaccination against yellow fever is required from travellers aged 9 months or over, arriving from countries with risk of yellow fever transmission, and for travellers having transited for more than 12 hours through an airport of a country with risk of yellow fever transmission.
- According to World Health Organization (WHO), from 11 July 2016 (for all countries), the yellow fever certificate will be valid for the duration of the life of the person vaccinated. As a consequence, a valid certificate, presented by arriving travellers, cannot be rejected on the grounds that more than ten years have passed since the date vaccination became effective as stated on the certificate; and that boosters or revaccination cannot be required.
- View the WHO list of countries with risk of yellow fever transmission.
- Proof of vaccination with the meningococcal quadrivalent vaccine (A, C, W, Y) is a visa requirement for Hajj and Umrah pilgrims and seasonal workers (see 'Some travellers' section below).
- Saudi Arabia have also listed other requirements for travellers visiting for Hajj and Umrah. Details are available from the Ministry of Health, in the Kingdom of Saudi Arabia Health Requirements and Recommendations for Travellers to Saudi Arabia for Hajj – 1445H (2024) and Health Requirements and Recommendations for Travellers to Saudi Arabia for Umrah - 1446H (2025).
Most travellers
The vaccines in this section are recommended for most travellers visiting this country. Information on these vaccines can be found by clicking on the blue arrow. Vaccines are listed alphabetically.
Tetanus
Tetanus is caused by a toxin released from Clostridium tetani bacteria and occurs worldwide. Tetanus bacteria are present in soil and manure and may be introduced through open wounds such as a puncture wound, burn or scratch.
Prevention
Travellers should thoroughly clean all wounds and seek medical attention for injuries such as animal bites/scratches, burns or wounds contaminated with soil.
Tetanus vaccination
- Travellers should have completed a tetanus vaccination course according to the UK schedule.
- If travelling to a country or area where medical facilities may be limited, a booster dose of a tetanus-containing vaccine is recommended if the last dose was more than ten years ago even if five doses of vaccine have been given previously.
Country-specific information on medical facilities may be found in the 'health' section of the FCDO foreign travel advice pages.
Tetanus in brief
Some travellers
The vaccines in this section are recommended for some travellers visiting this country. Information on when these vaccines should be considered can be found by clicking on the arrow. Vaccines are listed alphabetically.
Hepatitis A
Hepatitis A is a viral infection transmitted through contaminated food and water or by direct contact with an infectious person. Symptoms are often mild or absent in young children, but the disease can be more serious with advancing age. Recovery can vary from weeks to months. Following hepatitis A infection immunity is lifelong.
Prevention
All travellers should take care with personal, food and water hygiene.
Hepatitis A vaccination
Vaccination is recommended for those whose activities put them at increased risk. This includes:
- Those who are staying with or visiting the local population.
- Frequent and/or long-stay travellers to areas where sanitation and food hygiene are likely to be poor.
- Adventure travellers visiting rural areas and staying in basic accommodation such as backpackers.
- Those with existing medical conditions such as liver disease or haemophilia.
- Men who have sex with men.
- People who inject drugs.
- Those who may be exposed to the virus through their work.
- Those going to areas of hepatitis A outbreaks who have limited access to safe water and medical care.
Hepatitis A in brief
Hepatitis B
Hepatitis B is a viral infection spread through blood, semen and vaginal fluids. This mostly occurs during sexual contact or as a result of blood-to-blood contact (for example from contaminated equipment during medical and dental procedures, tattooing or body piercing procedures, and sharing of intravenous needles). Mothers with the virus can also pass on the infection to their baby during childbirth.
Hepatitis B in Saudi Arabia
This country is considered to have an intermediate or high prevalence of hepatitis B.
Prevention
Travellers should avoid contact with blood or body fluids. This includes:
- Avoiding unprotected sexual intercourse.
- Avoiding tattooing, piercing, public shaving, and acupuncture (unless sterile equipment is used).
- Not sharing needles or other injection equipment.
- Following universal precautions if working in a healthcare or other higher risk setting.
A sterile medical equipment kit may be helpful when travelling to resource poor areas.
Hepatitis B vaccination
Vaccination could be considered for all travellers and is recommended for those whose activities or medical history put them at increased risk. This includes:
- Those who may have unprotected sex.
- Those who may be exposed to contaminated needles through injecting drug use.
- Those who may be exposed to blood or body fluids through their work (e.g. health and aid workers).
- Those at high risk of requiring medical or dental procedures or hospitalisation e.g. those with pre-existing medical conditions, those who may require travelling for medical care abroad, or those travelling to visit families or relatives.
- Long-stay travellers.
- Those who are participating in contact sports.
- Families adopting children from this country.
Hepatitis B in brief
Meningococcal disease
For Hajj and Umrah pilgrims and seasonal workers to this area, proof of vaccination with a meningococcal ACWY vaccine is a visa requirement for entry.
Meningococcal disease is a bacterial infection transmitted by inhaling respiratory droplets or direct contact with respiratory secretions from an infected person. This is usually following prolonged or frequent close contact. The most common forms of meningococcal disease are meningococcal meningitis (infection of the protective lining around the brain) and septicaemia (blood poisoning).
Hajj and Umrah pilgrims and seasonal workers at the pilgrimages are at increased risk due to the crowded conditions and possible close contact with people from countries with higher rates of meningococcal disease.
Meningococcal disease in Saudi Arabia
Outbreaks of meningococcal meningitis were reported in 1987, 2000 and 2001 during the Hajj.
Prevention
Travellers may reduce their risk by avoiding overcrowded situations where possible.
Meningococcal disease vaccination
For pilgrims and seasonal workers proof of vaccination with a meningococcal ACWY vaccine is a visa requirement for entry. When the meningococcal ACWY conjugate vaccine is used, this should be given at least 10 days before, and within the last 5 years of planned travel. Details of the vaccine name and type (i.e. conjugate vaccine) should be recorded in a patient held vaccine record showing the traveller’s full name. It is advisable that this vaccination record is issued by the traveller's doctor, nurse or pharmacist and should reflect accurately details of the vaccine administered and be authenticated with the healthcare providers official stamp.
Pilgrims and seasonal workers must carry vaccination certificates with them for inspection by the Saudi Authority at port of entry.
The meningococcal ACWY conjugate vaccine is recommended. If a polysaccharide ACWY vaccine has been administered previously (no longer available in UK) it should have been administered within the last 3 years of planned travel.
Meningococcal disease in brief
Rabies
Rabies is a viral infection which is usually transmitted following contact with the saliva of an infected animal most often via a bite, scratch or lick to an open wound or mucous membrane (such as on the eye, nose or mouth). Although many different animals can transmit the virus, most cases follow a bite or scratch from an infected dog. In some parts of the world, bats are an important source of infection.
Rabies symptoms can take some time to develop, but when they do, the condition is almost always fatal.
The risk of exposure is increased by certain activities and length of stay (see below). Children are at increased risk as they are less likely to avoid contact with animals and to report a bite, scratch or lick.
Rabies in Saudi Arabia
Rabies is considered a risk and has been reported in domestic animals in this country. Bats may also carry rabies-like viruses.
Prevention
- Travellers should avoid contact with all animals. Rabies is preventable with prompt post-exposure treatment.
- Following a possible exposure, wounds should be thoroughly cleansed and an urgent local medical assessment sought, even if the wound appears trivial.
- Post-exposure treatment and advice should be in accordance with national guidelines.
Rabies vaccination
A full course of pre-exposure vaccines simplifies and shortens the course of post-exposure treatment and removes the need for rabies immunoglobulin which is in short supply world-wide.
Pre-exposure vaccinations are recommended for travellers whose activities put them at increased risk including:
- those at risk due to their work (e.g. laboratory staff working with the virus, those working with animals or health workers who may be caring for infected patients).
- those travelling to areas where access to post-exposure treatment and medical care is limited.
- those planning higher risk activities such as running or cycling.
- long-stay travellers (more than one month).
Rabies in brief
Malaria
Malaria is a serious illness caused by infection of red blood cells with a parasite called Plasmodium. The disease is transmitted by mosquitoes which predominantly feed between dusk and dawn.
Symptoms usually begin with a fever (high temperature) of 38°C (100°F) or more. Other symptoms may include feeling cold and shivery, headache, nausea, vomiting and aching muscles. Symptoms may appear between eight days and one year after the infected mosquito bite.
Prompt diagnosis and treatment is required as people with malaria can deteriorate quickly. Those at higher risk of malaria, or of severe complications from malaria, include pregnant women, infants and young children, the elderly, travellers who do not have a functioning spleen and those visiting friends and relatives.
Prevention
Travellers should follow an ABCD guide to preventing malaria:
Awareness of the risk – Risk depends on the specific location, season of travel, length of stay, activities and type of accommodation.
Bite prevention – Travellers should take mosquito bite avoidance measures.
Chemoprophylaxis – Travellers should take antimalarials (malaria prevention tablets) if appropriate for the area (see below). No antimalarials are 100% effective but taking them in combination with mosquito bite avoidance measures will give substantial protection against malaria.
Diagnosis – Travellers who develop a fever of 38°C [100°F] or higher more than one week after being in a malaria risk area, or who develop any symptoms suggestive of malaria within a year of return should seek immediate medical care. Emergency standby treatment may be considered for those going to remote areas with limited access to medical attention.
Risk areas
- There is a low risk of malaria in the south western provinces of Saudi Arabia, along the border with Yemen including Asir province below 2,000m: awareness of risk and bite avoidance recommended.
- There is no risk in the cities of Jeddah, Makkah (Mecca), Medina, Riyadh, and Ta’if, or in Asir province above 2,000m: bite avoidance only recommended.
Special risk groups
In low risk areas, antimalarials may be considered in exceptional circumstances for travellers who are at higher risk of malaria (such as long term travellers visiting friends and relatives), or of severe complications from malaria (such as the elderly [over 70 years], the immunosuppressed,those with complex co-morbidities, pregnant women, infants and young children). The final decision whether or not to advise antimalarials rests with the travel health advisor and the traveller after individual risk assessment.
Travellers with an absent or poorly functioning spleen should be dissuaded from travel to any area with risk of malaria. Where travel is essential, awareness, rigorous bite avoidance and antimalarials should be advised, even for the low risk areas.
For special risk groups, you may wish to seek specialist advice. For the low risk areas in this country/area, atovaquone/proguanil OR doxycycline OR mefloquine would be suitable options.
Antimalarial recommendations map
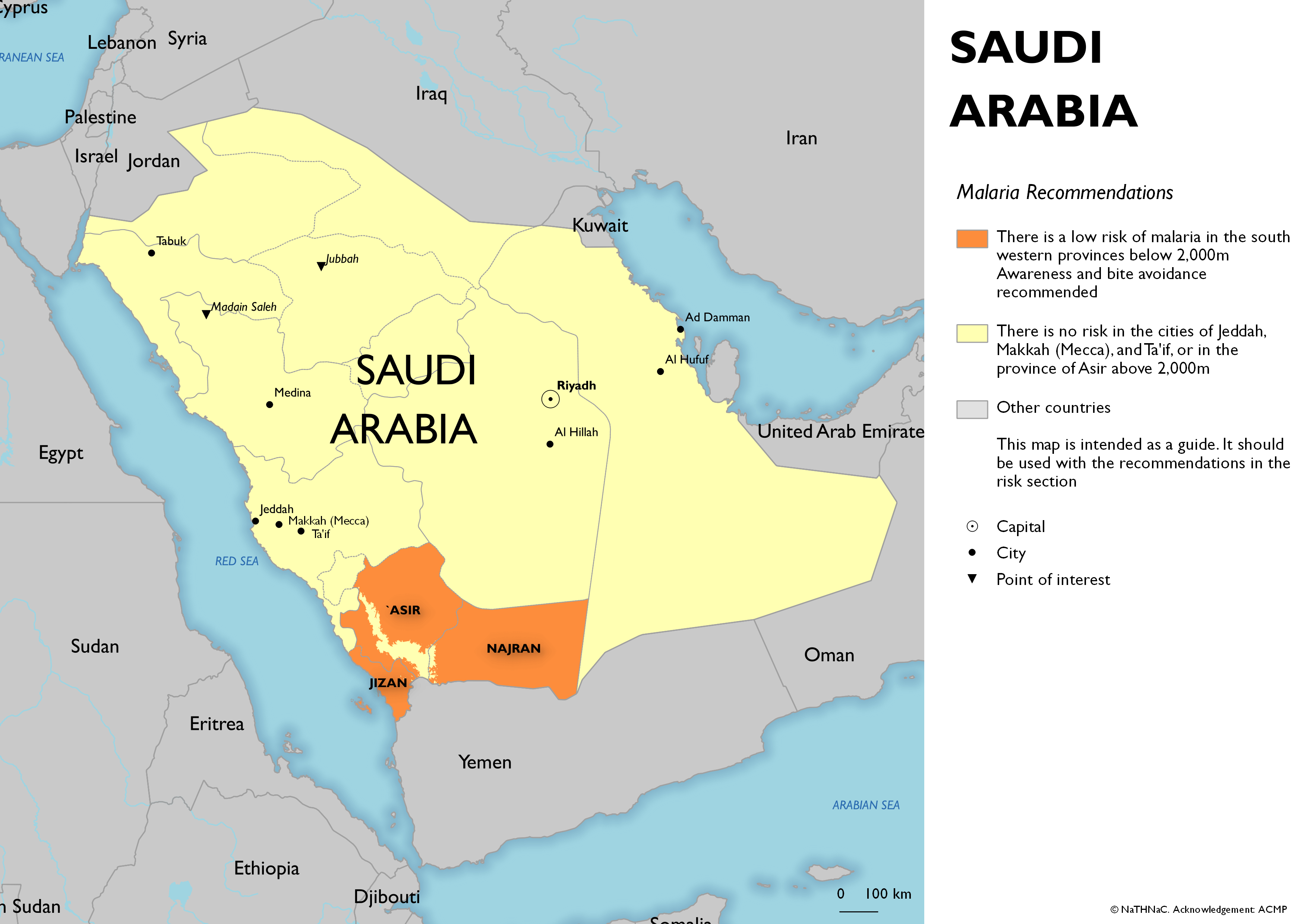
- Click on map to open in a new window
Resources
Other Risks
There are some risks that are relevant to all travellers regardless of destination. These may for example include road traffic and other accidents, diseases transmitted by contaminated food and water, sexually transmitted infections, or health issues related to the heat or cold.
Some additional risks (which may be present in all or part of this country) are mentioned below and are presented alphabetically. Select risk to expand information.
Altitude
There is a risk of altitude illness when travelling to destinations of 2,500 metres (8,200 feet) or higher. Important risk factors are the altitude gained, rate of ascent and sleeping altitude. Rapid ascent without a period of acclimatisation puts a traveller at higher risk.
There are three syndromes; acute mountain sickness (AMS), high-altitude cerebral oedema (HACE) and high-altitude pulmonary oedema (HAPE). HACE and HAPE require immediate descent and medical treatment.
Altitude illness in Saudi Arabia
There is a point of elevation in this country higher than 2,500 metres.
Prevention
- Travellers should spend a few days at an altitude below 3,000m.
- Where possible travellers should avoid travel from altitudes less than 1,200m to altitudes greater than 3,500m in a single day.
- Ascent above 3,000m should be gradual. Travellers should avoid increasing sleeping elevation by more than 500m per day and ensure a rest day (at the same altitude) every three or four days.
- Acetazolamide can be used to assist with acclimatisation, but should not replace gradual ascent.
- Travellers who develop symptoms of AMS (headache, fatigue, loss of appetite, nausea and sleep disturbance) should avoid further ascent. In the absence of improvement or with progression of symptoms the first response should be to descend.
- Development of HACE or HAPE symptoms requires immediate descent and emergency medical treatment.
Altitude illness in brief
Biting insects or ticks
Insect or tick bites can cause irritation and infections of the skin at the site of a bite. They can also spread certain diseases.
Diseases in Western Asia
There is a risk of insect or tick-borne diseases in some areas of Western Asia. This includes diseases such as chikungunya, Crimean-Congo haemorrhagic fever, leishmaniasis, Rift Valley fever and West Nile virus.
Prevention
- All travellers should avoid insect and tick bites day and night.
- There are no vaccinations (or medications) to prevent these diseases.
Further information about specific insect or tick-borne diseases for this country can be found, if appropriate on this page, in other sections of the country information pages and the insect and tick bite avoidance factsheet.
Dengue
Dengue is a viral infection spread by mosquitoes which mainly feed during daytime hours. It causes a flu-like illness, which can occasionally develop into a more serious life-threatening illness. Severe dengue is rare in travellers.
The mosquitoes that spread dengue are more common in towns, cities and surrounding areas.
There is a risk of dengue in the provinces of Al Madinah, Jizan and Makkah (including the cities of Mecca and Jeddah).
Dengue in Saudi Arabia
Prevention
- Travellers should avoid mosquito bites particularly during daytime hours.
- A dengue vaccine is licensed in the UK for the prevention of dengue disease in individuals from 4 years of age. The Joint Committee on Vaccination and Immunisation (JCVI) and World Health Organization are in the process of reviewing the product information. Recommendations on the use of this vaccine will be published in due course.
Dengue in brief
Influenza
Seasonal influenza is a viral infection of the respiratory tract and spreads easily from person to person via respiratory droplets when coughing and sneezing. Symptoms appear rapidly and include fever, muscle aches, headache, malaise (feeling unwell), cough, sore throat and a runny nose. In healthy individuals, symptoms improve without treatment within two to seven days. Severe illness is more common in those aged 65 years or over, those under 2 years of age, or those who have underlying medical conditions that increase their risk for complications of influenza.
Seasonal influenza in Saudi Arabia
Seasonal influenza occurs throughout the world. In the northern hemisphere (including the UK), most influenza occurs from as early as October through to March. In the southern hemisphere, influenza mostly occurs between April and September. In the tropics, influenza can occur throughout the year.
Prevention
All travellers should:
- Avoid close contact with symptomatic individuals
- Avoid crowded conditions where possible
- Wash their hands frequently
- Practise ‘cough hygiene’: sneezing or coughing into a tissue and promptly discarding it safely, and washing their hands
- Avoid travel if unwell with influenza-like symptoms
- A vaccine is available in certain circumstances (see below)*
*In the UK, seasonal influenza vaccine is offered routinely each year to those at higher risk of developing of severe disease following influenza infection, and certain additional groups such as healthcare workers and children as part of the UK national schedule (see information on vaccination). For those who do not fall into these groups, vaccination may be available privately.
If individuals at higher risk of severe disease following influenza infection are travelling to a country when influenza is likely to be circulating they should ensure they received a flu vaccination in the previous 12 months.
The vaccine used in the UK protects against the strains predicted to occur during the winter months of the northern hemisphere. It is not possible to obtain vaccine for the southern hemisphere in the UK, but the vaccine used during the UK influenza season should still provide important protection against strains likely to occur during the southern hemisphere influenza season, and in the tropics.
Avian influenza
Avian influenza viruses can rarely infect and cause disease in humans. Such cases are usually associated with close exposure to infected bird or animal populations. Where appropriate, information on these will be available in the outbreaks and news sections of the relevant country pages. Seasonal influenza vaccines will not provide protection against avian influenza.
Avian influenza in brief
Middle East respiratory syndrome coronavirus
MERS-CoV is a viral infection spread by direct or indirect contact with infected camels or camel-related products. Limited person to person transmission through coughing and sneezing from infected persons, typically in healthcare settings, has also been reported.
Symptoms include fever and cough that can progress to severe shortness of breath and breathing difficulties. Deaths have been reported, with the risk increasing with advancing age or underlying medical conditions.
Middle East respiratory syndrome coronavirus in Saudi Arabia
MERS-CoV has been reported to occur in this country.
Prevention
All travellers, particularly those with chronic medical conditions, should practise good general health measures, such as regular hand washing with soap and water at all times, but especially after visiting farms, barns or market areas. They should:
- Avoid contact with camels.
- Avoid raw camel milk and/or camel products.
- Avoid consumption of any type of raw milk, raw milk products and any food that may be contaminated with animal secretions, unless peeled and cleaned and/or thoroughly cooked.
There is currently no vaccine to prevent MERS-CoV.
More information about Hajj and Umrah is available from the Hajj and Umrah factsheet.
MERS-CoV in brief
Outdoor air quality
Poor air quality is a significant public health problem in many parts of the world. Exposure to high levels of air pollution over short time periods (e.g. minutes/hours/days) and longer time periods (e.g. years) is linked to many different acute and chronic health problems. These effects are mainly on the respiratory (lungs and airways) and cardiovascular (heart function and blood circulation) systems.
Current information on world air quality is available from the world air quality index project.
Prevention
Travellers with health problems that might make them more vulnerable to the effects of air pollution who are travelling to areas of high pollution should:
- discuss their travel plans with their doctor, and carry adequate supplies of their regular medication.
- take sensible precautions to minimise their exposure to high levels of air pollution.
- check local air quality data and amend their activities accordingly.
- take notice of any health advisories published by the local Ministry of Health and Department for Environment, and follow the guidance provided.
It is unclear if face masks are beneficial at reducing exposure and may make breathing more difficult for those with pre-existing lung conditions. Those who choose to use one should make sure that the mask fits well and know how to wear it properly.
Outdoor air quality in brief
Schistosomiasis
Schistosomiasis is a parasitic infection. Schistosoma larvae are released from infected freshwater snails and can penetrate intact human skin following contact with contaminated freshwater. Travellers may be exposed during activities such as wading, swimming, bathing or washing clothes in freshwater streams, rivers or lakes.
Schistosomiasis infection may cause no symptoms, but early symptoms can include a rash and itchy skin ('swimmer's itch'), fever, chills, cough, or muscle aches. If not treated, it can cause serious long term health problems such as intestinal or bladder disease.
Schistosomiasis in Saudi Arabia
Cases of schistosomiasis have previously been reported from this country. There is a very low risk of schistosomiasis in this country.
Prevention
- There is no vaccine or tablets to prevent schistosomiasis.
- All travellers should avoid wading, swimming, or bathing in fresh water. Swimming in adequately chlorinated water or sea water is not a risk for schistosomiasis.
- Drink water that is boiled, filtered or bottled.
- Application of insect repellent before exposure to fresh water, or towel drying after possible exposure to schistosomiasis are not reliable in preventing infection.
- If you have concerns about your risk discuss with your health care provider.
Schistosomiasis in brief
News

Middle East respiratory syndrome coronavirus (MERS-CoV) reminder
NaTHNaC has reviewed MERS-CoV advice for UK travellers in line with current UK Health Security Agency recommendations and is reminding travellers to be aware of their MERS-CoV risk

Hajj 1445H and Umrah update: 2024
Information for pilgrims planning to perform Hajj or Umrah in 2024

Malaria: a reminder for travellers over the winter holiday season
Advice for travellers and health professionals about malaria
Outbreaks
Using information collated from a variety of sources, we regularly review and update information on overseas disease outbreaks and other health issues that may affect the UK traveller.
Please note that not all cases of disease or outbreaks are reported; some diseases may only be reported if they occur outside of the usual recognised risk area or season, or they have been reported in greater than usual numbers.
Further information on the Outbreak Surveillance section.
Meningococcal disease in Saudi Arabia
As of 21 June 2024, a total of 14 cases of invasive meningococcal disease (serogroup W) have been reported in the United States (5), France (4), the United Kingdom (3), Norway (1), and the Netherlands (1) in travellers or contacts of travellers returning from Umrah pilgrimage in Saudi Arabia.
Map

